Disease overview
Mycosis fungoides (MF) is a rare form of T-cell (white cell – lymphocytes) lymphoma of the skin (cutaneous).1
Lymphocytes are a type of white blood cell in the lymph system, part of your immune system.2 They live in the lymph nodes (small collections of immune cells) and in other lymphoid tissue, such as the spleen, skin and bone marrow.2
T-cell lymphocytes fight foreign bacteria and activate your immune system. T-cells also help clean up the foreign bacteria after an immune response. 2
With MF, the T-cells become malignant (cancerous) and affect your skin.1,2
MF progresses slowly and unpredictably over years, from patches to more infiltrated plaques and eventually to tumours.3
The prognosis of patients with MF is dependent on stage, and in particular the type and extent of skin lesions and the presence of extracutaneous manifestations of the disease. Patients with limited patch stage MF have a similar life expectancy to an age-, sex-, and race-matched control population. 10-year disease-specific survivals were 83% for patients with generalized patch/plaque disease (covering more than 10% of the skin surface), 42% for patients with tumour stage disease, and about 20% for patients with histologically documented lymph node involvement.3
Although it is the most common subtype of CTCL, MF is considered a rare disease and typically affects older adults: the median age at diagnosis is around 55-60 years, with a male-to-female ratio of 2/1: it can however affect even children and adolescents (Figure 1).4
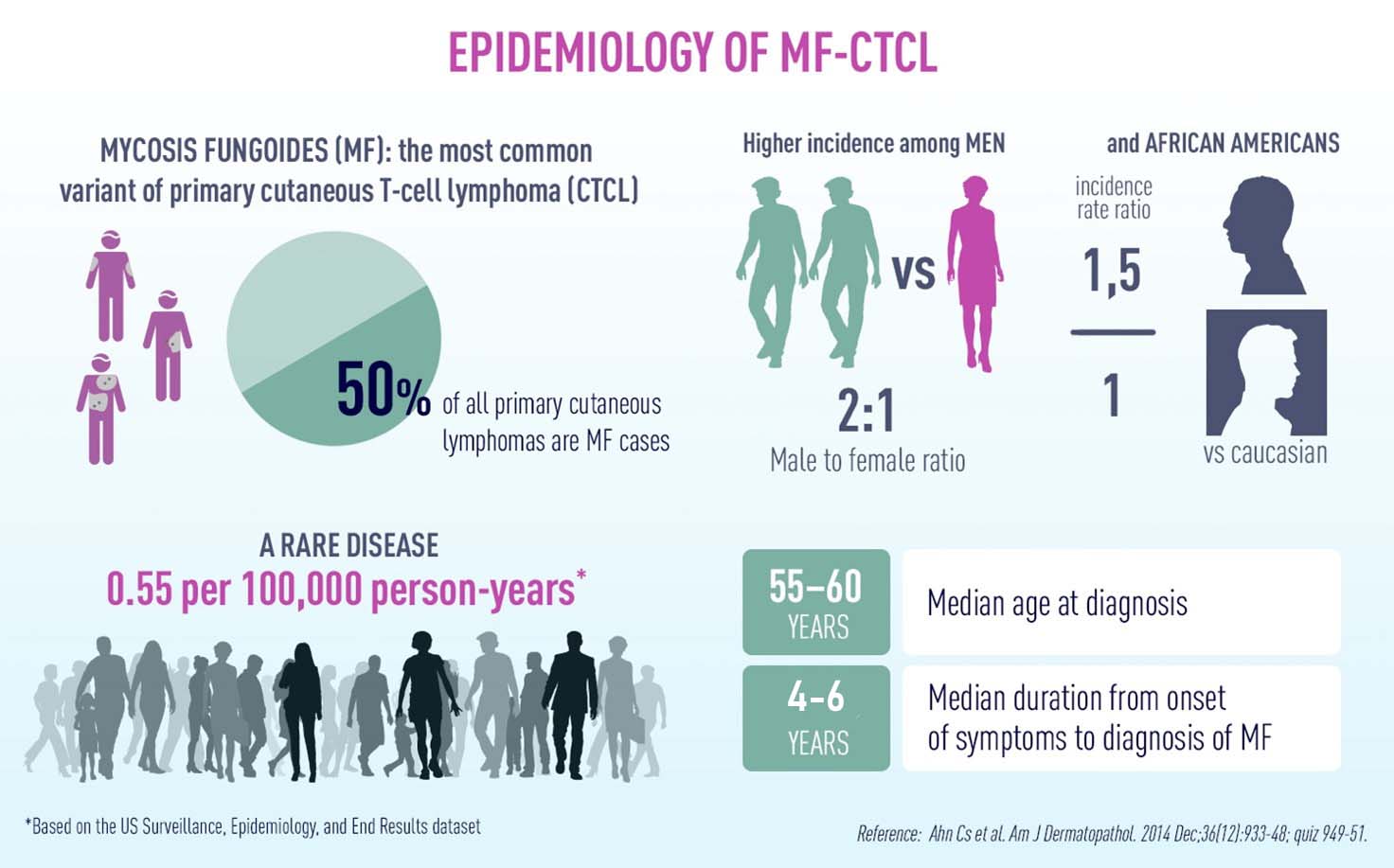
Figure 1. MF-CTCL in numbers.
Symptoms
Mycosis fungoides symptoms occur in several phases of skin changes.
For many people, the first sign of disease is a mycosis fungoides rash. Mycosis fungoides stages include:2
- Premycotic phase: A scaly, symptom-free skin rash. This rash appears in areas of the body not usually exposed to the sun.
- Patch phase: The skin around the rash becomes thin. It may be itchy and dry, like eczema.
- Plaque phase: Your skin forms papules (small raised bumps) or lesions (hard bumps).
- Tumour phase: Tumours form on your skin. They may develop ulcers and get infected.
Causes
The exact cause of mycosis fungoides is not known. Current theories include antigen persistence, retroviruses (e.g., HTLV-1, etc.), and exposure to cancer-causing (carcinogenic) substances.1
Diagnosis
A diagnosis of mycosis fungoides may be made by a thorough clinical evaluation and a variety of specialized techniques and tests including histology, DNA cytophotometry, nuclear contour analysis, and analysis of T-cell receptor gene rearrangement.1